
Carpal (wrist) Trauma
The carpus (wrist) is a complex structure made up of multiple
bones
ligaments
joint spaces
The carpus is an important part of the front leg as it absorbs force from the front half of the body (60% of total body weight) and converts this into forward movement, much like a spring. Injury often comes due to chronic repetitive over-use (sporting animals) OR due to acute over-loading (falling or jump trauma).
What is CARPAL HYPEREXTENSION?
With carpal hyperextension, the patient develops collapse of the carpus where the wrist joint drops and gets closer to the ground.
What causes carpal hyperextension?
We frequently see this condition as a result of trauma. The patient traps the front paw and over stretches the carpus. This can result in stretching or tearing of the ligaments at the back of the joint (palmar ligaments) which are vital for the stability of the joint. Once the ligaments are torn, they cannot be repaired. Equally, stretched ligaments show poor healing and the carpus is often damaged permanently.
What are the signs?
Limping will develop in the front legs. With trauma, usually only one limb is affected, however, during a fall both the front limbs can be involved. The carpus will drop towards the ground, meaning the standing angle at the front of the joint rather than being 140° – 180° in dogs and 160° – 180° in cats, decreases and can be reduced to 90° in the most severe cases. This change presents as an almost L-shaped appearance to the joint. Swelling and pain may also develop.
How is it diagnosed?
Clinical examination is an invaluable part of identifying the abnormality - often swelling, pain and abnormal movement is detected. In order to accurately diagnose the severity of the problem, stressed radiographs are performed under sedation or anaesthesia.

Normal stressed extension response on the left image, with the 3 joint levels identified in blue. The 3 joint levels from top to bottom include: radial-carpal, inter-carpal and carpal-metacarpal.
Abnormal stressed extension response on the right image.
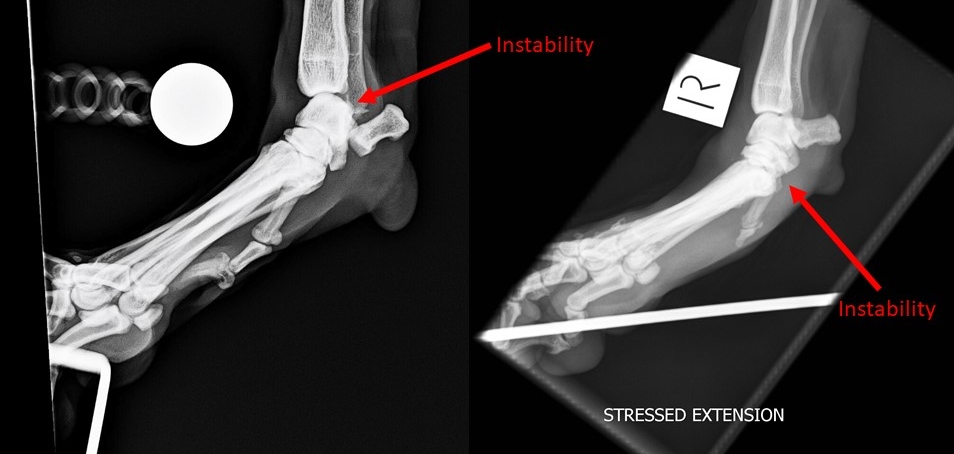
Abnormal extension at the radial-carpal joint on the left image. Abnormal extension at the carpal-metacarpal joint on the left image.
How is the injury treated?
Given the poor healing potential of the supportive palmar ligaments, this condition responds poorly to non-surgical treatment. Splinting and support dressing can provide some stability in the short term, but longer term results are poor as the ligaments fail to heal. Given the poor results with conservative care, surgery is often the treatment of choice.
Surgical management?
Surgery using arthrodesis (fusing of the joint) is often recommended. This can be where the whole joint is fused, called pancarpal arthrodesis, or where part of the joint is fused, called partial carpal arthrodesis.
Arthrodesis aims to eliminate pain and allow the patient to use the limb comfortable. During this procedure, the cartilage from the entire joint is removed and the carpus is stabilised with a bone plate or sometimes two plates and screws. A bone graft (bone harvested from the shoulder on the same side to provide cells and healing potential) is placed at the arthrodesis site to stimulate healing.

Recovery
Careful rest after fracture surgery is the key to success. Patients will remain hospitalised for between 1-3 days post operatively depending on comfort, mobility and temperament. Once they are ready for home management, a dedicated rehabilitation and activity plan will be put in place.
Key elements of home management during the first 6 weeks include:
Room or cage confinement during unsupervised periods
Non slip flooring
Leash controlled walking activity
Patients progress will be reviewed at 2 time points:
10-14 days after surgery for a progress check and suture removal
6 weeks after surgery for additional assessment and follow-up radiographs to assess rate of healing. This check is very important to guide further activity, a return to normal activity is sometimes possible at this time.
Potential complications?
Complications following this procedure are not uncommon (up to 20% of cases) but are usually able to be resolved. These may be minor complications requiring limited treatment or more severe requiring further surgical management. Complications include: infection, failure of the carpus to fuse, seroma formation and fracture. Complications can be minimised when the surgery is performed by a surgical specialist with significant experience in advanced orthopaedics.
Outcome
Many dogs will return to normal or near normal function after this procedure, albeit with an altered gait. There is some straightening of the leg and more movement that occurs at the toes but this is very well tolerated.
The video below shows the outcome after a single session, bilateral pancarpal arthrodesis was performed by Dr Beierer on a most lovely dog named Macca.

Typical appearance after complete wrist fusion on the left leg, whilst the right leg demonstrates normal foot appearance.